Meeting Global Radiotherapy Demand with AI
Cancer incidence is rising fast, radiation oncology teams are under growing pressure, and equipment shortages persist in many parts of…
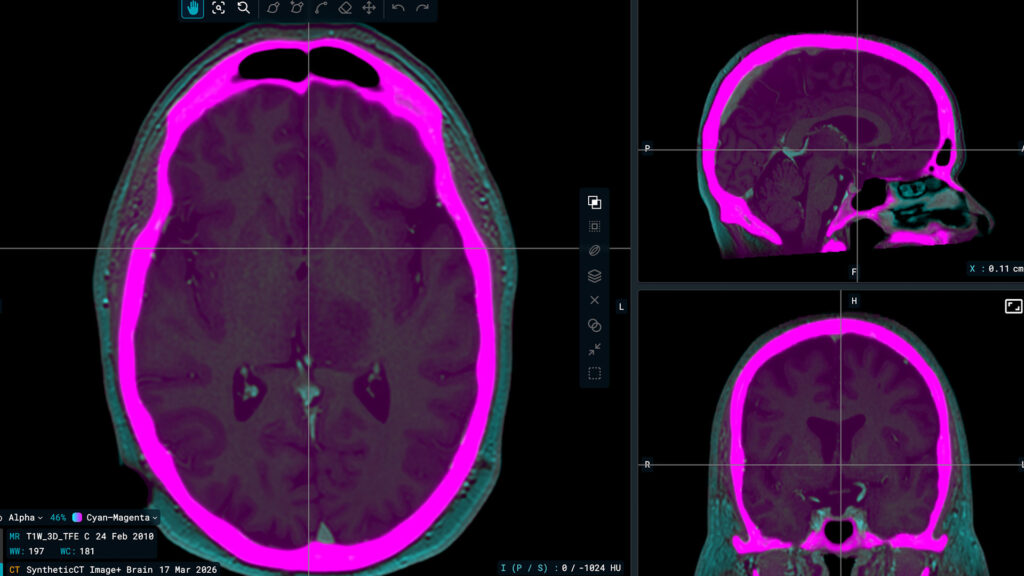
TYKS is one of the first centres in the world to use synthetic CT generated from MRI. What has that experience taught you about the technology?
When we started using it, it was genuinely new technology, and the image quality at that time was not as good as it is today. We had to put in more effort to make it work clinically, and there was a learning process involved. But since then the evolution has been towards better and better synthetic CT, and I think nowadays the images are quite close to conventional CT — they are easier to use and easier to integrate clinically.
But I think the bigger advantage is that, for most cases in the pelvis and brain, MRI is already needed for target delineation. When we generate synthetic CT from MRI, we need only the MRI — we can skip the CT entirely. The key benefit of that, particularly in the pelvic area, is that we no longer need to perform image registration between CT and MRI. That registration always carries some error, because the organs are in a slightly different position between scan sessions.
When assessing whether a synthetic CT solution is ready for clinical use, what does ‘clinical-grade’ actually mean to you?
First of all, the synthetic CT has to be reliable. There should be no significant errors in the generated image — it should not introduce structures that are not there, and it should not omit structures that are important. If either of those things happens, it is simply not reliable enough for clinical use.
The geometric accuracy also has to be correct. For dose calculation, the body outline and anatomical dimensions must be right. And the quality of the source MRI matters — the MRI image quality has to be good enough, and the geometry of the MRI has to be correct, because the synthetic CT is derived from it.
There is also a practical side to acceptance. CT is what clinicians are used to seeing, so the closer the synthetic CT resembles conventional CT in appearance, the easier it is to take into clinical use. And there is one more consideration: nowadays almost all treatments are positioned using CBCT, and the synthetic CT serves as the reference image on the treatment machine during that CBCT registration. So image quality in the synthetic CT is also critical for correct patient positioning at each treatment fraction.
Can you walk us through the evaluation you did on Image+ — what were you looking at, and what did the results show?
I want to be clear that this was a first-impression evaluation, not a full clinical verification — a more thorough study is still ongoing. With that said, the first impression was that the image quality is quite good — good enough, I would say. One observation is that the AI tends to smooth organ borders slightly more than you would see in conventional CT, but not to a degree that is problematic.
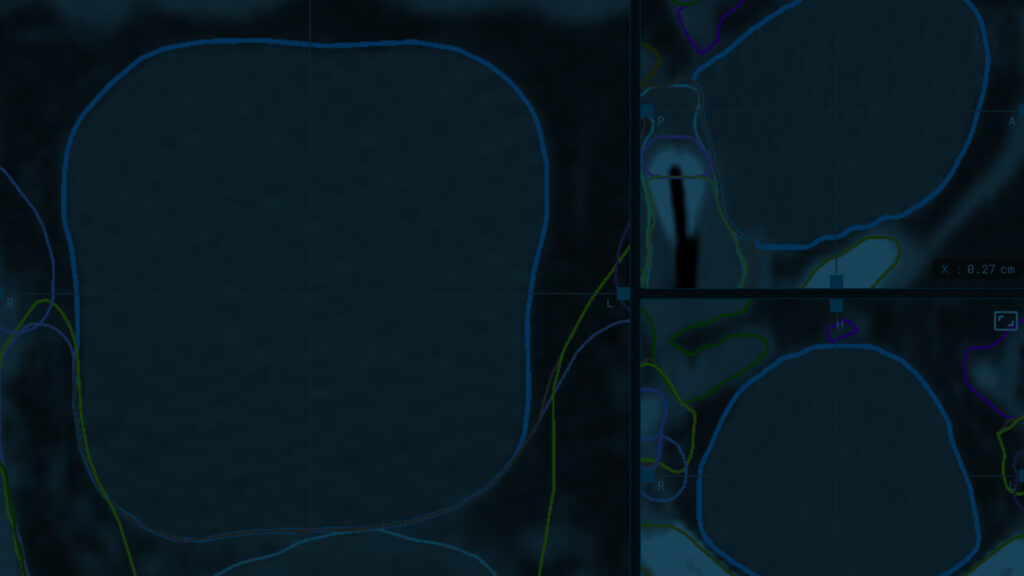
The significant potential advantage for us is that Image+ generates synthetic CT from T2-weighted MRI, whereas our current clinical workflow uses T1-weighted images. For pelvic cases, T2 images are already used for contouring and target definition in almost every case. So if the synthetic CT is also based on those same T2 images, the target structures — the prostate, for example — are well aligned between the synthetic CT and the images used for contouring. That is an improvement over the current situation, where T1 is used for synthetic CT and T2 for target definition.
How important is it to have tools like contouring, synthetic imaging, and dose prediction in one platform rather than in separate systems?
It would make things considerably easier, and automation is an important goal in radiotherapy treatment planning today. If all of those steps — synthetic CT generation, auto-segmentation, dose prediction, and treatment plan generation — are on a single platform, it becomes possible to fully automate the planning process.
The vision is that when the images are acquired, a treatment plan is already being generated. Of course, that plan would need to be verified and most likely corrected in some areas, but at least there would be a solid starting point ready.
What are the main technical challenges that still need to be addressed?
The challenge with using T2-weighted images for pelvic synthetic CT is that you need rather high spatial resolution for target delineation as well as full transaxial body outline and sufficient cranial-caudal coverage for dose calculation. Processing a very large number of voxels translated into longer generation times than would be practical for clinical use. This is something that will need to be addressed as the workflow moves towards routine clinical implementation — synthetic CT needs to be available within minutes.
Where do you see the collaboration with MVision going, and what would a successful Workspace+ implementation look like for TYKS?
The collaboration gives us access to state-of-the-art tools for clinical testing and for taking new capabilities into use. What we are working towards is the automation of the treatment planning process, and that is what Workspace+ makes possible.
More specifically, one goal is to implement T2-based pelvic synthetic CT clinically. Although we already have a well-functioning T1-based synthetic CT solution, using T2 images for both contouring and synthetic CT generation would be a benefit — it means the same image set serves both purposes.
Another step would be to take synthetic CT generated from CBCT into clinical use for offline adaptive treatment planning. Currently we use CBCT for verification and monitoring, but not for treatment planning. Image+ could be a good tool to expand that use. And looking further ahead, if the planning and automation processes become fast enough, this kind of approach could eventually support online adaptive treatment on standard linear accelerators — not just on dedicated adaptive systems. That is where the technology is heading, and it is something we want to be part of.
I would also say that for centres that are considering MRI-only treatment planning or synthetic CT workflows, this would be a good option to explore — particularly for those who are just starting out with this kind of technology.
About Turku University Hospital
Turku University Hospital (TYKS) provides specialised medical care for the residents of Southwest Finland and also delivers university-level services for the regions of Satakunta and Vaasa. It employs around 8,000 people and offers a wide range of clinical services and training opportunities. Founded in 1756, TYKS is one of the oldest hospitals in Northern Europe and continues to serve as a major academic and clinical centre in Finland.
*CE-marked (CE 2797) medical device under EU MDR 2017/745; Workspace+ is not available in all markets.