We are here to explore topics around AI in radiotherapy, share practical tips, and address questions as well as biases we with our partners come across in our daily work.
Prone position is a body position where one is lying down on the stomach with the chest down and back up. While body positions may seem irrelevant in cancer care, it is actually an important detail in radiotherapy treatment.
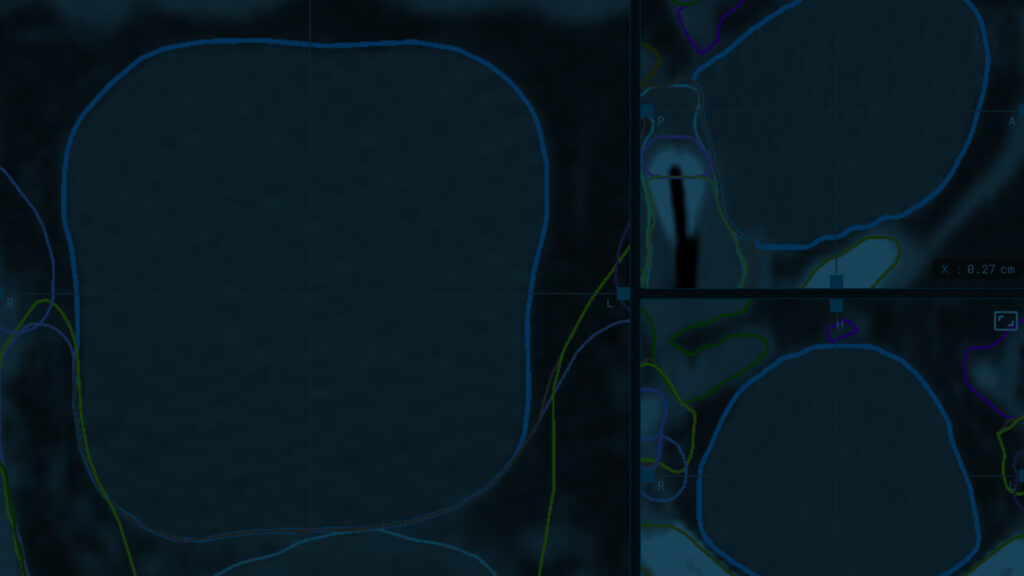
A vital part of the treatment workflow and planning is imaging, a procedure where the patient’s body is scanned. An example of this is computerized tomography, or CT, scan that combines a series of X-ray images taken from different angles around the body and uses computer processing to create cross-sectional images of the bones, blood vessels as well as soft tissues inside the body. These images known as slices are then viewed by clinicians to gain an understanding of the tumor placement and size as well as the location of healthy tissues around it. The clinicians draw these out on the images, a procedure known as contouring. One could say, these images and lines on them create the map for the whole radiotherapy treatment plan.
When we move, our organs do too. And so does a potential tumor. Since our bodies are not made of cement, our tissues are placed differently also when lying down – whether that is on our backs or stomachs. While most of the imaging happens with patients lying on their backs with chests up, in the supine position, it is not always the best option or simply possible. This is when prone comes to the picture.
While it is not necessarily a common practice, a case where the prone position could be used is for scanning a breast cancer patient. The position can help to displace the breast tissue more significantly away from the chest wall and torso. This can furthermore help to make a more accurate treatment plan to minimize normal tissue doses and treatment toxicity. In other words, the clinician would have a clearer image to use as the map for the treatment itself.
As quite often in life, the specific terms do not play the key role – only what actually happens does. While it may sound simple to just take for example a CT scan in the prone position and proceed to contour, it can be difficult to find and draw the needed organs in this position. Simply because it is not usual and not as well practiced as the more common, supine position.
Fortunately, AI can help.
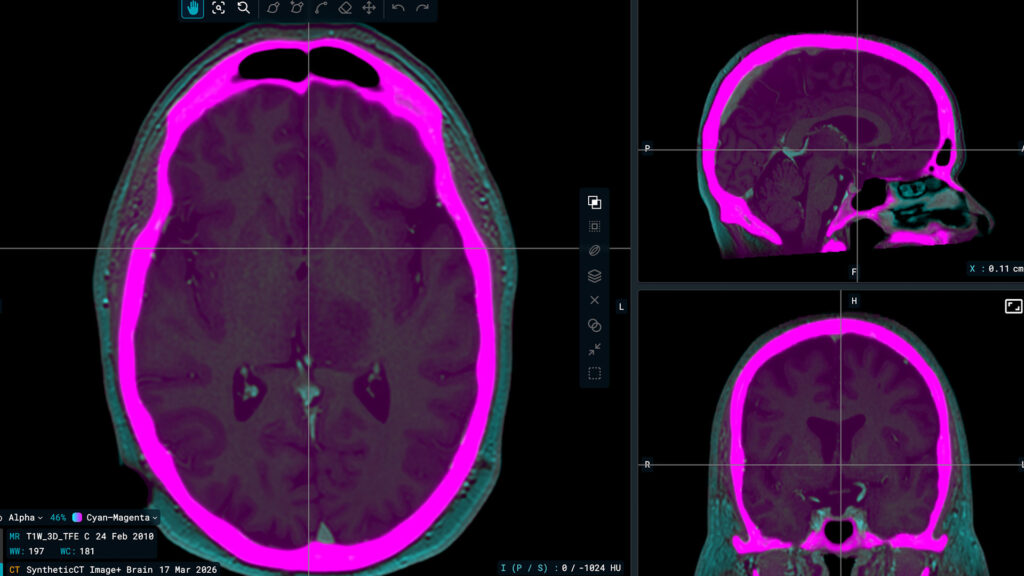
An auto-contouring tool powered by AI, such as MVision Segmentation Service, does contours for both supine and prone positions. While it indeed is wonderful that an algorithm can help with prone position contouring, the importance of the logic this demonstrates is even greater. It shows that a state-of-the-art algorithm can indeed adapt to uncommon circumstances. In other words, it teaches and corrects itself. So, as long as the information that is fed to the system is correct, an auto-contouring software could ideally make high-quality contours with a patient in any given position.
Why is this important?
The ability to do auto-contours on prone positions as easily as supine gives clinicians more options. In other words, a patient who cannot lie on the back, can now be scanned on the stomach without this lengthening the planning process which would potentially happen if the clinician was not used to contouring rare prone position images. All the clinician needs to do is to let an auto-contouring solution draw and simply check the results.
This influences also research. If one dives deeper into the concept of prone position in radiotherapy, there is no one clear result or finding but rather a set of individual studies that are not necessarily scientifically comparable. Some support the use of prone position for contouring of specific organs while others have not found any significant impact. There are also papers that do not recommend the use of prone position. The contouring styles are simply not the same style or otherwise in line. This potentially prevents the research from going forward. By using a state-of-the-art auto-segmentation, researchers can conduct studies that are more comparable – also in prone position.
Read more about prone position:
Gonzalez VJ, Hullett CR, Burt L, Rassiah-Szegedi P, Sarkar V, Tward JD, Hazard LJ, Huang YJ, Salter BJ, Gaffney DK. Impact of prone versus supine positioning on small bowel dose with pelvic intensity modulated radiation therapy. Adv Radiat Oncol. 2017 Jan 24;2(2):235-243. doi: 10.1016/j.adro.2017.01.005. PMID: 28740937; PMCID: PMC5514253..
Pinkawa M, Gagel B, Demirel C, Schmachtenberg A, Asadpour B, Eble MJ. Dose-volume histogram evaluation of prone and supine patient position in external beam radiotherapy for cervical and endometrial cancer. Radiother Oncol. 2003 Oct;69(1):99-105. doi: 10.1016/s0167-8140(03)00244-5. PMID: 14597362.
Koelbl O, Richter S, Flentje M. Influence of patient positioning on dose-volume histogram and normal tissue complication probability for small bowel and bladder in patients receiving pelvic irradiation: a prospective study using a 3D planning system and a radiobiological model. Int J Radiat Oncol Biol Phys. 1999 Dec 1;45(5):1193-8. doi: 10.1016/s0360-3016(99)00345-4. PMID: 10613312.